Quick answer: Scientists at MIT engineered white-footed mice to resist Lyme, so in lab studies, ticks feeding on them picked up far less of the bacteria. If it works in the wild, it could mean fewer infected ticks over time, and eventually fewer human cases, though that is not yet proven. It does not treat anyone who already has Lyme, and it is years from any wider release. For an existing infection, care still depends on accurate testing and treatment matched to the case.
Scientists at MIT engineered mice that fight off Lyme and pass that protection to their pups. In a 2026 study, ticks that fed on these mice picked up almost no Lyme. It is a real step toward fewer infected ticks, but it does little for anyone who already has it.
If you are living with Lyme right now, the limit matters more than the promise. The research is still worth knowing: it targets one of the most efficient ways ticks get infected, and over time it could mean fewer people get Lyme, or fewer who live with the worry of getting it again.
This article covers what the MIT mouse research did, why Lyme has been so hard to stop, what the science does and does not change for people who are sick now, and what care for established Lyme looks like with a Lyme-literate team in the DC area.
Deer are not where ticks pick up Lyme, and that is exactly why MIT went after mice. The tick that spreads it is the deer tick, so the name points the finger at deer. Adult ticks do feed on deer, and deer move ticks across the landscape and drive up their numbers. What deer do not do is carry the Lyme bacterium in a form that infects a feeding tick.
White-footed mice are the most studied carrier, and they pass Lyme to 40 to 90 percent of the young ticks that bite them, which then carry it on to whatever they bite next, sometimes a person. They are not the whole story. Shrews and chipmunks carry Lyme too, and in some places shrews may account for even more infected ticks than mice. Lower how much Lyme any one of these animals carries, and you weaken a link in the chain, though never the only one.

They used CRISPR, the gene-editing tool, to give mice a built-in defense against Lyme, one they carry into the next generation without further engineering. That is the work behind Mice Against Ticks, a project from Kevin Esvelt's lab at MIT. In the study published in Nature Communications in April 2026, engineered lab mice resisted infection, and ticks feeding on them rarely picked up the bacteria, while ordinary mice passed it to most of theirs. The same group has since built the tools to do this in the white-footed mouse, a main driver of Lyme in the wild.
They also built in a brake, and it came straight from what the affected communities asked for. Residents worried about releasing engineered animals into the wild, so the team used only white-footed mouse DNA and skipped the aggressive version of this technology, the kind that drives a change through a whole population fast and is hard to undo. The trait is designed to spread slowly, so researchers and residents can watch for problems before it goes anywhere widely. A plan people can watch as it unfolds is one a town can vote yes to.
Lyme has had an open road for years. It is the most common tick-borne disease in the country, and about 476,000 Americans are diagnosed and treated for it each year, while around 89,000 cases are formally reported to the CDC.
The reason it is hard to treat sits in the same gap that let it spread. A single tick often carries more than Lyme, passing along co-infections like Babesia or Bartonella that each behave differently and need their own plan.
Testing is the next problem, because the standard test misses at both ends of the illness. It looks for your body's antibody response to Lyme, not the bacteria. Early on, before that response has formed, standard two-tier testing caught just 22 to 36 percent of early cases in one 2026 study, and the CDC's own journal reports sensitivity of 30 to 40 percent during early infection. At the other end, that 2026 study found the antibody response often never develops after antibiotic treatment, so a negative result does not always rule Lyme out. People fall through at both ends.
The bacteria can also be hard to reach. Over time, the Lyme bacteria may shelter in biofilms, protective layers that can blunt the effect of antibiotics, something researchers have mostly seen in lab and animal studies. That is one reason the usual few weeks of antibiotics, the right tool for a fresh bite, can fall short of an illness that has been building for years.
In our practice, the patients who reach us have usually done everything the standard path asked of them and stayed sick anyway. More of them now carry a co-infection no one thought to test for.
The enemy here was never one doctor, but a system built to treat a fresh bite and little else. It leaves the people already sick to hear that their tests are normal and their symptoms are stress, then offers them no way forward. And it never went after Lyme where it starts, in the animals no one treats and the ticks no one stops. So if you were told to wait it out, you were reading the situation correctly.
The research works out in the wild rather than in your bloodstream, so it offers little for the infection you already carry. Even in the best case it faces years of testing and monitoring before any wider release, with the project's own roadmap laying out the steps still ahead. Any rollout would begin in New England, well before the mid-Atlantic. For anyone sick today, this moves the science, not the next twelve months.
What it moves is still worth watching. Targeting the animal that infects the ticks is a different premise than Lyme prevention has run on before. This spring it produced results clear enough to publish, though whether it lowers human cases across a region is a question the work has not answered yet. For patients long told the illness was not real, a research effort years in the making says otherwise, and if the approach works at scale, being treated once may no longer mean waiting for the next bite.
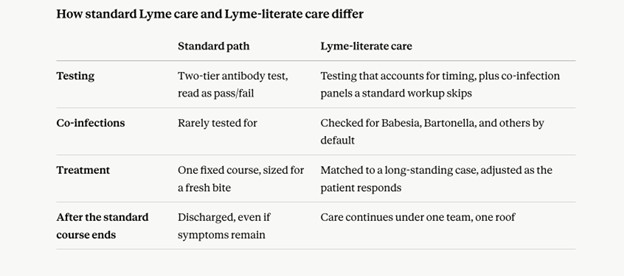
MIT is working on how Lyme spreads. Our Lyme care is the other half, treating it in the person who has it now, which for established Lyme is the part most patients have been missing. It starts with testing that accounts for timing and looks for the co-infections a standard panel does not check for, including for the patient who already has a co-infection diagnosis but no plan that holds all of it together. From there, treatment gets matched to a long-standing case rather than a fresh bite, and adjusted as the patient responds, instead of running one fixed course and discharging when the weeks are up.
At Indigo, every Lyme patient is seen by our Clinical Director, Snejana Sharkar, FNP, RND, ACNP, who is trained for the complexity these cases carry. Testing, treatment planning, supplements, and IV therapy happen under one roof with one team, so the patient follows one plan instead of coordinating it herself.
"Somebody giving you a diagnosis which is the worst news in your life but also saying I've seen this a million times, I've built it back up a million times, you kind of go okay, then I can surrender to that."
Indigo patient, Washington DC
Patient experiences are individual, and results vary.
If you are sick now, the next move is a conversation, not more waiting. The prevention research is worth following, and it will not reach the mid-Atlantic for years.
Most people who come to us have spent years being told their labs look normal, or handed diagnoses that never added up to a plan. The gap is usually in what was tested and when, and in the co-infections a standard panel skips. Indigo has done this work across DC, Maryland, and Virginia since 2011, with more than 3,500 patients and Lyme care led by a clinician experienced in complex chronic illness.
A complimentary Discovery Call is where every Indigo patient starts. It is a 20-minute phone call, and a team member walks through your symptom history, your past testing, and what you have already tried. You come away with a clear read on whether your Lyme case is one we can help with, and what a fuller workup would look for. No cost, no commitment, just a straight answer on whether this is worth pursuing.
This content is provided by Indigo Integrative Health Clinic for educational purposes only. It does not constitute medical advice, a diagnosis, or a treatment recommendation, and does not establish a provider-patient relationship. Individual health conditions vary — information presented here may not apply to your specific situation. Always consult a qualified, licensed healthcare provider before making decisions about your health, medications, supplements, or treatment plan.

Lyme disease shares key symptoms with fibromyalgia, multiple sclerosis, and chronic fatigue syndrome, so it can be mistaken for any of them. It is also over-diagnosed in people who do have one of those conditions. The honest answer is that Lyme is worth confirming or ruling out with a knowledgeable clinician, not assumed in either direction.
Most people leave a Hashimoto's diagnosis with a prescription and no explanation for why it started. You are told your immune system is attacking your thyroid, and that you will likely take levothyroxine for life. What you are rarely told is why this started now, when other people carry the same risk genes and never get sick.
Scientists at MIT engineered mice that fight off Lyme and pass that protection to their pups. In a 2026 study, ticks that fed on these mice picked up almost no Lyme. It is a real step toward fewer infected ticks, but it does little for anyone who already has it.
Hours of Operation
Monday - Friday
9am - 5pm

